How ineffective are current Alzheimer’s disease treatments? Quite. So much so, in fact, that David Cameron, the Conservative former prime minister of the United Kingdom – a supposed BFF of Big Business and one can only deduce, Big Pharma – called out the pharmaceutical industry for its “failures undermining dementia research and drug development.” A huge multi-billion-dollar industry being called out by a world leader isn’t something that happens every day.
But then again, Cameron’s sentiments have plenty of merits. Per Scientific American, dementia drug research has failed miserably. In a mega-study investigating 244 drugs across 413 clinical trials, researchers found that just one drug was approved. In other words, 99.6 percent of the experiments amounted to nothing. Just this past January, another company discontinued not one but two Alzheimer’s drugs during the final stages of clinical trials.
So, what is going on? Well, it’s one thing for a politician to lambast an industry for their lack of progress and next-to-nil results; it’s quite another to pinpoint and act upon the catalysts of dementia. It certainly doesn’t help that the drug industry is so entrenched into the health care apparatus either, as this discourages looking at alternative methods of care. Mix in public ignorance about natural remedies (yes, including marijuana) and the outlook doesn’t appear favorable.
But researchers may just be edging ever closer to a real solution to the Alzheimer’s problem – and it isn’t in the form of an expensive pill. What is it, then? Well, if studies are to be believed, it’s the use of cannabis.
In this article, we’re going to discuss some interesting findings concerning the use of cannabis and Alzheimer’s disease. We’ll briefly touch on the problem of Alzheimer’s in today’s society as well as the problems posed by conventional dementia treatments.
Alzheimer’s Disease: An Overview
Alzheimer’s disease is a progressive neurodegenerative disease characterized by a gradual loss of memory, learning ability, communication, and judgment. In some cases, these cognitive functions decline to a point where the person becomes entirely dependent on caregivers for daily activities.
Alzheimer’s is typically found in those over the age of 65, of whom approximately 1 in 14 adults are affected. The highest concentration of patients with the disease are those over the age of 80, with 1 in every 6 meeting the criteria for diagnosis. This type of Alzheimer’s, also known as Late-onset Alzheimer’s is the most common, accounting for nearly 90 percent of all cases.
Only 6 to 8 percent of patients develop symptoms before the age of 65 – a condition known as early-onset Alzheimers – with those affected having a family history of the disease.
The rarest form of Alzheimer’s is called Familial Alzheimer’s disease (FAD), which is believed to be wholly inherited. In affected families, members of at least two generations are found to have had Alzheimer’s disease. FAD accounts for less than 1 percent of all Alzheimer’s cases.
Alzheimer’s disease symptoms are classified into three categories: mild, moderate, and severe.
Common symptoms of mild Alzheimer’s include:
- Difficulty completely once-routine tasks
- Impaired sense of judgment
- Impaired sense of direction or getting lost
- Increased anxiety and aggression
- Lethargy and lack of purpose
- Memory loss
- Monetary difficulties
- Poor decision making
- Repeating the same questions
Moderate symptoms include:
- All of the symptoms mentioned above
- Further deterioration of memory
- Poor judgment and worsening confusion
- Requiring assistance when doing simple tasks (e.g. bathing, grooming, using the bathroom.)
- Significant changes in personality and behavior.
Severe symptoms may include:
- All of the signs mentioned above
- Losing the ability to converse or speak
- Complete dependence on others for many tasks
- Declining physical abilities (e.g. inability to walk or sit up straight, rigid muscles, etc.)
Problems Abound With Dementia Drugs
It’s not just that so few drugs are approved for Alzheimer’s and other forms of dementia; the problem is also that they are ineffective and downright counterproductive in just about every conceivable way. Let us briefly discuss the problems with current dementia treatment.
They’re expensive
First, Alzheimer’s prescription drugs are costly. While Medicaid covers much of the costs, prescription drugs for dementia can add up to hundreds of dollars per month. For seniors who live on a fixed income, this amount may be unattainable, forcing them to choose drugs over other necessities like food, or vice-versa.
They carry nasty side effects
Among the pervasive side effects of dementia medicines are abdominal cramps, bruising, confusion, constipation diarrhea, insomnia, muscle cramps, nausea, vomiting, fatigue, and weight loss.
They’re ineffective (except for one)
While the statistics may vary, they seem to agree on this point: Alzheimer’s prescription medications aren’t very effective at doing what they say they’ll do. In a meta-analysis of 41 randomized control trials published in Alzheimer’s Research & Therapy, the research team concludes that there is not one drug that reduces neuropsychiatric symptoms of Alzheimer’s.
Memantine is the sole dementia medication that carries significant benefits. In both the previous meta-analysis, and the second analysis of 30 studies published in the Journal of Alzheimer’s Disease, memantine (brand name “Namenda”) significantly improved learning, cognition, and memory. (Furthermore, compared with the other type of dementia medications – acetylcholinesterase inhibitors [e.g. donepezil] – memantine has relatively few and less severe side effects.)
Cannabis as an Alzheimer’s and Dementia Treatment
“When we investigated the power of THC … we found that [it] was a very effective inhibitor of acetylcholinesterase. [We] also found that THC was considerably more effective than two of the approved drugs…” – Kim Janda, Ph.D. (source)
It’s a good thing that marijuana use is becoming less and less taboo – especially for those with medical conditions. To give you an idea of just how widespread cannabis is as either a primary or secondary treatment option, consider what it’s been thought to help treat:
- Alzheimer’s disease (of course!)
- Anxiety
- Cancer (by killing cancer cells and slowing tumor growth)
- Chron’s disease
- Chronic pain
- Eating disorders
- Epilepsy
- Excessive weight loss (in people with AIDS and cancer)
- Glaucoma
- Inflammation
- Loss of appetite
- Mental health conditions such as schizophrenia and posttraumatic stress disorder (PTSD)
- Nausea and vomiting (from chemotherapy)
- Multiple sclerosis (MS)
- Muscle spasms
Understanding Alzheimer’s
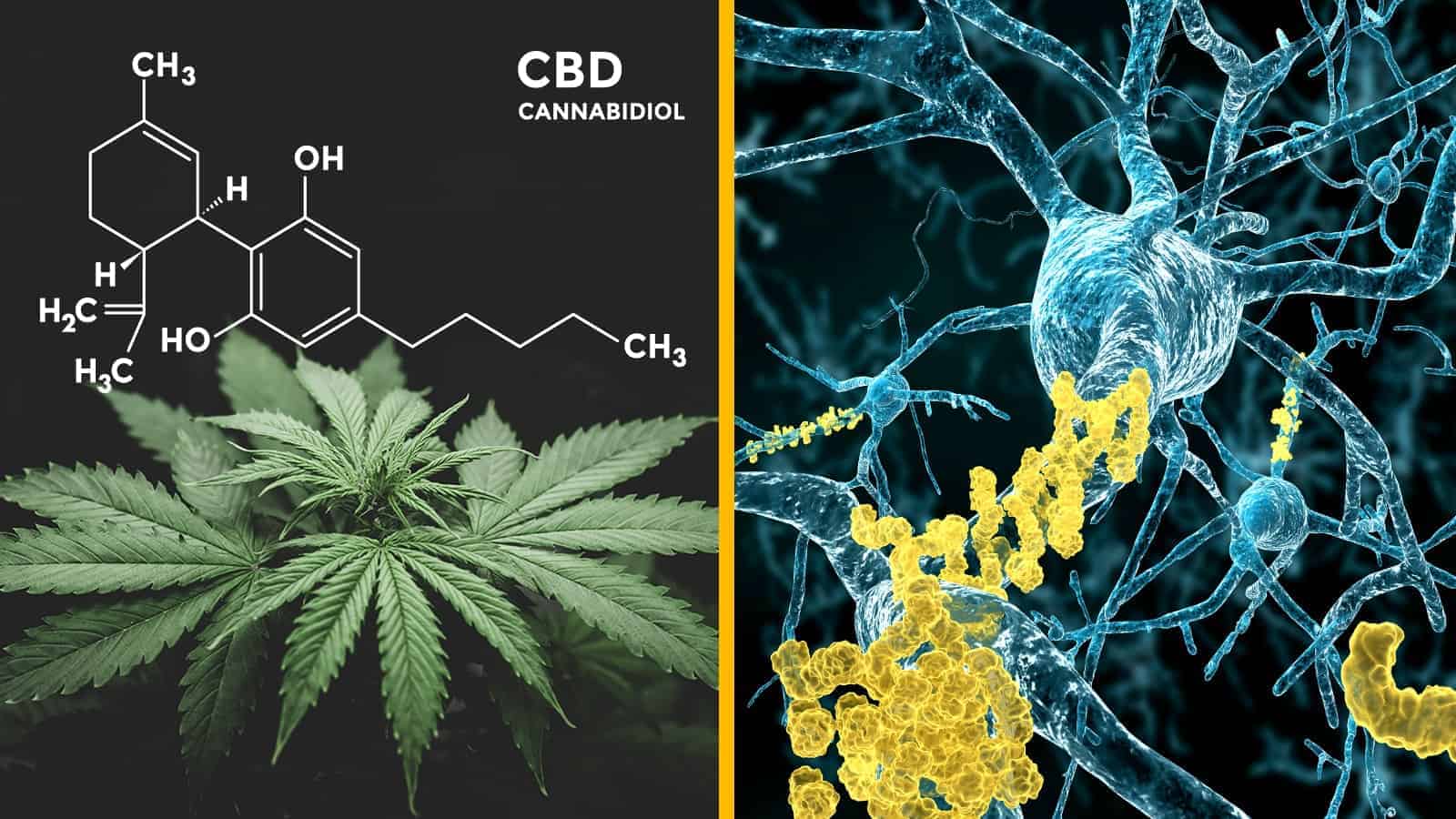
To understand how cannabis may help treat Alzheimer’s, we must first understand the underlying neurophysiology of the disease. To this point, researchers attribute the onset and progression of the disease to the buildup of a sticky plaque protein called beta-amyloid. It is thought that the protein disrupts communication between neurons in the brain and causes cellular death. It is these effects of the beta-amyloid, neuroscientists say, that causes both the cognitive and neuropsychiatric problems seen in Alzheimer’s patients.
An active compound in marijuana called tetrahydrocannabinol (THC) may help to remove the toxic buildup of beta-amyloid, say researchers from the Salk Institute for Biological Studies in California. Moreover, THC may also help to reduce inflammation in nerve cells. Dave Schubert, the leading neurobiologist at the institute, believes that his team’s study is the first of its kind to demonstrate these dual properties of THC.

Schubert’s team may have made another novel finding: the inflammation produced in the brain may stem from beta-amyloid buildup within the neurons – not immune-like cells within the brain as thought previously. Moreover, “THC-like compounds (within) the nerve cells themselves may be involved in protecting the cells from dying,” says Antonio Currais, a researcher in Shubert’s lab.
Schubert’s team attributes these the anti-inflammatory, beta-amyloid reduction properties to THC to activation of the brain’s “switches,” or receptors. Research has shown that endocannabinoids activate these receptors, causing intracellular signaling within the brain. As THC has similar molecular activity as endocannabinoids, they have similar effects of the brain’s receptors.
Final Thoughts
In related research, Schubert’s lab discovered that a potential drug known as J147 produces similar effects of beta-amyloid proteins and reduces the inflammatory response in the brain. Schubert’s team has found that the J147 drug works by manipulating a mitochondrial protein called ATP, which performs the role of providing cellular energy to neurons. As of this writing, J147 is said to be nearing clinical trials – the first step, albeit a long one, in gaining approval for mass manufacturing and distribution.
As of this writing, the Salk Institute is advancing its research on THC and endocannabinoids as a potential Alzheimer’s treatment.